

MTIMA Launches a Four-Month Cardiology Lecture Series—Built for Malawi, Tuned to the Clinic
On an August evening in Blantyre—morning in Toronto—the grid of faces steadies and the chat quiets. A cursor finds the mic, a slide advances, and the first ECG tracings appear like staves of music. This is MTIMA’s Cardiology Lecture Series, built for clinic days rather than conference halls, and it moves with the rhythm of work: brisk, clear, and aimed at the next patient.
Running from August through November 2024, the series convenes seven voices with reach and range—Drs. Michael Hammer, Keith Kwok, Rishi Bhargava, Kareem Morant, Carlos Fernando, joined by Dr. David McCarty and Rianne de Bruin-Bon—to teach what matters most in Malawi’s case mix: electrocardiography that avoids false alarms, heart failure that can’t wait until Thursday, rheumatic heart disease that hides in plain sight, cardiomyopathies that confound a busy ward, and right-heart assessment that changes triage. The brief is simple and unsentimental: make decisions faster and safer.
The rooms are virtual, but the stakes are not. Each session draws more than 30 Malawian clinicians—clinical officers, nurses, trainees—who bring clinic questions rather than conference questions. The hour is part tutorial, part rehearsal: a tricky apical view becomes a moment of shared craft; a muddled ECG becomes a clean call; a guideline is translated into three steps someone can take tomorrow. Slides give way to problem-solving; teaching notes land in inboxes before the night is over.
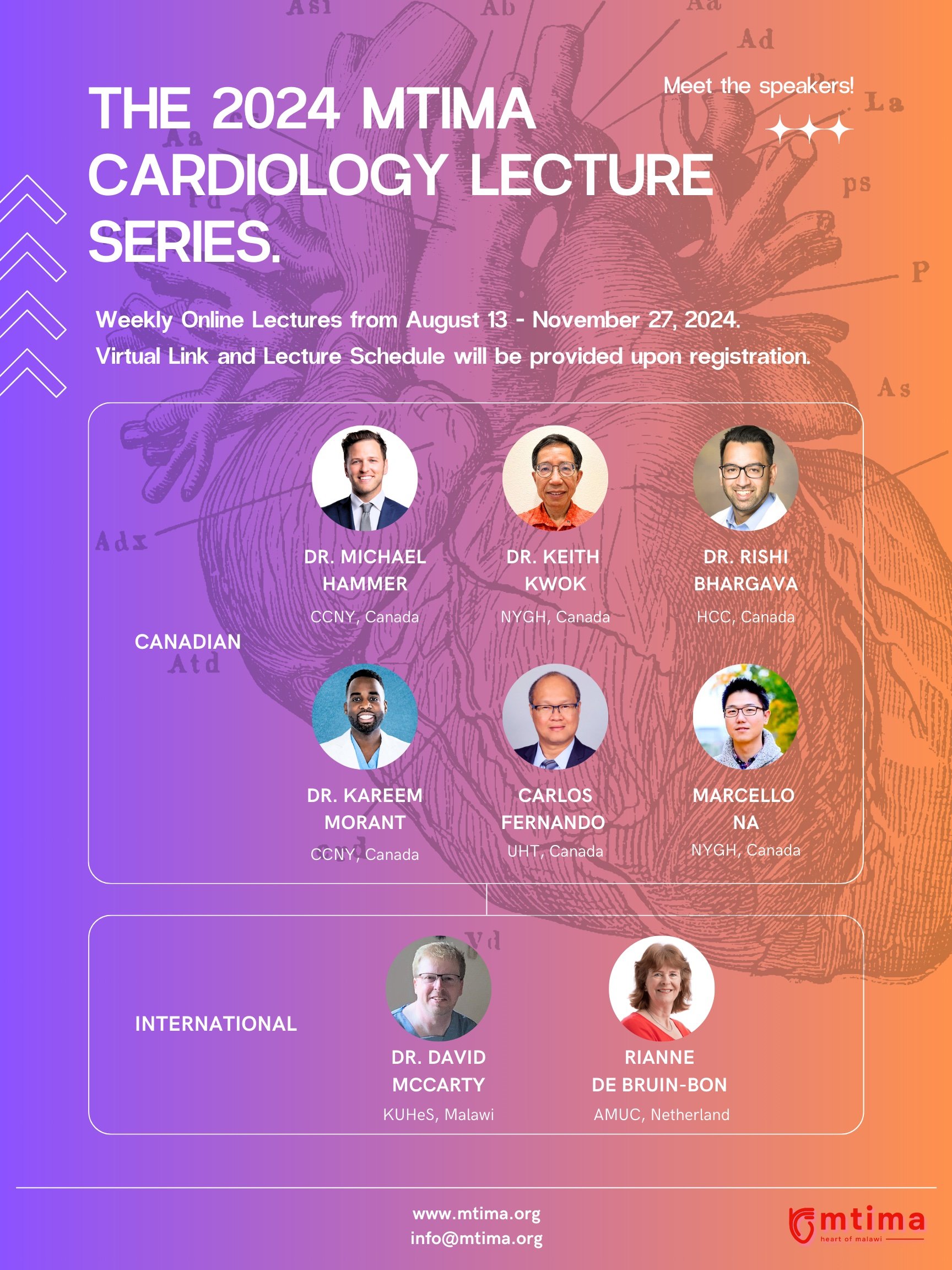
Guest Speakers
Across weeks, a pattern emerges. When ECGs are read with discipline, referrals stop drifting. When echo measurements are reproducible, repeat scans fall away. When rheumatic valve disease is recognized earlier, surgery lists hold room for those who truly need them. The impact is quiet, the kind that rarely trends: a queue that moves, a ward that breathes, a clinician who goes home less uncertain than they arrived.
The format matters. By meeting online, the series sidesteps the usual frictions—travel budgets, visas, days away from wards—without sacrificing the feeling of a room. Materials are practical, cases are local, and the tone is collegial rather than ornamental. No one is here to impress a podium; everyone is here to improve a Tuesday.

Guest Speakers’ Topics
What lingers after the sign-off isn’t a headline but a habit: evidence turning into muscle memory. A clinician sees a pattern faster. A report is written with one fewer hedge. A patient gets where they need to go without a second visit. Multiply that by weeks and names on the attendance list, and you have the shape of progress—incremental, cumulative, and owned by the people who do the work.
By November, the series will end; the ripple will not. The notes, the recordings, the small changes that add up—those stay behind. And that, more than any single slide, is the point: not to perform expertise at a distance, but to leave skill in local hands.