

Radiology, Rewired: Malawi’s Plan to See Patients Clearly
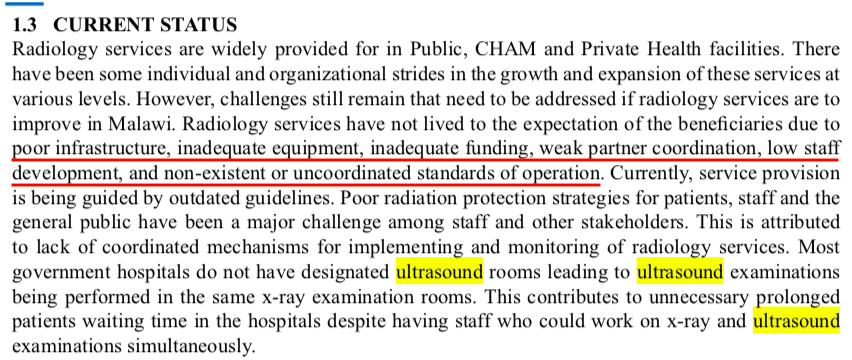
At a district hospital on the Shire plain, a clinician weighs two imperfect options: send a patient home on guesswork, or treat blind and hope for the best. The X-ray unit is down again. The ultrasound machine works, but trained hands are scarce. In settings like this, imaging isn’t a luxury add-on; it’s the difference between precision and probability.
Malawi’s National Radiology Policy sets out to close that gap. Its premise is blunt and overdue: quality medical imaging is essential care, not a nice-to-have. Poor radiology isn’t merely inconvenient—it cascades. Patients receive the wrong treatments, stay sicker for longer, spend money they don’t have, lose income, and lose faith in the health system. On the public side, weak imaging wastes scarce resources on ineffective care and robs the economy of productivity through avoidable illness and death.
The policy’s purpose is unifying rather than flashy: create one guiding framework to standardize and raise the quality of diagnostic, interventional, and therapeutic imaging across the country. That means clear rules for what services belong at each level of care, from health centres to central hospitals, and a consistent standard for how images are acquired, read, reported, and acted upon. It aligns with Malawi’s Health Sector Strategic Plan II (2017–2022) and the National Health Policy—both aimed at delivering an Essential Health Package without pushing families into financial ruin.
Many Malawian healthcare practitioners continue to rely on outdated medical knowledge, which may impact the quality of patient care.
The scale of the human-resource challenge is stark. As of 2020, the public sector counted 96 radiography technicians, 9 radiation therapists, 30 diagnostic radiographers, 1 sonographer, and 1 radiologist—serving a population of more than 17 million. Mission and private facilities added 71 more staff, but the numbers remain thin. Training has historically plateaued at diploma level, with only a handful holding bachelor’s degrees and just one trained in ultrasonography. A second degree-granting school has opened, with the first graduates expected in 2021—a start, not a finish.
Why the urgency? Because modern medicine runs on pictures. Tuberculosis or heart failure, trauma or stroke, cancer or obstetric emergency—each demands the right image at the right time, interpreted by someone who knows what to look for and what to do next. The policy’s writers name the missing specialties plainly: ultrasonography, MRI, interventional imaging, nuclear medicine, mammography, and more. In other words, not just more imaging, but better imaging—and across the full spectrum of disease.

What will it take to move from paper to practice?
Standards by level of care. A clear, realistic menu for each facility tier prevents both overreach and neglect.
Training pipelines. Degree programs and in-service upskilling must produce not only more practitioners but also supervisors, educators, and managers who can sustain quality.
Maintenance and uptime. Machines that work only on payday are no machines at all; service contracts and spare-parts logistics are as important as procurement.
Quality assurance. Protocols, peer review, and structured reporting keep images actionable—and patients safer.
Financing with protection. Public provision should remain free at point of care, while partnerships avoid nudging the poorest patients to the margins.
This is also a cardiac story. Malawi’s burden of non-communicable disease is rising, and cardiovascular disease is threaded through clinics from Blantyre to Mzuzu. Echocardiography—portable, powerful, and comparatively affordable—sits on the front line. When sonographers can reliably acquire standard views and when reports are clear, heart-failure patients reach diuretics and follow-up faster; suspected valve disease is escalated appropriately; unnecessary transfers shrink.
Here, organizations like MTIMA fit the policy’s blueprint. The work is deliberately unglamorous: hands-on echo training, measurement discipline, simple reporting templates, and case reviews that catch errors before they harden into habit. The payoff is quiet but cumulative—fewer repeat scans, cleaner referrals, earlier interventions. Each improvement frees minutes in a clinic day and beds on a ward. When minutes and beds compound, systems breathe.

Malawian students used a low-cost portable ultrasound for rural healthcare and training.
Malawi’s National Radiology Policy does not promise instant transformation. It offers something sturdier: a plan to align every stakeholder—public, mission, private, academic—around the same standard of visibility. See better, decide faster, treat smarter. In a system where exam rooms often double as classrooms, that’s not just policy language. It’s a survival strategy.